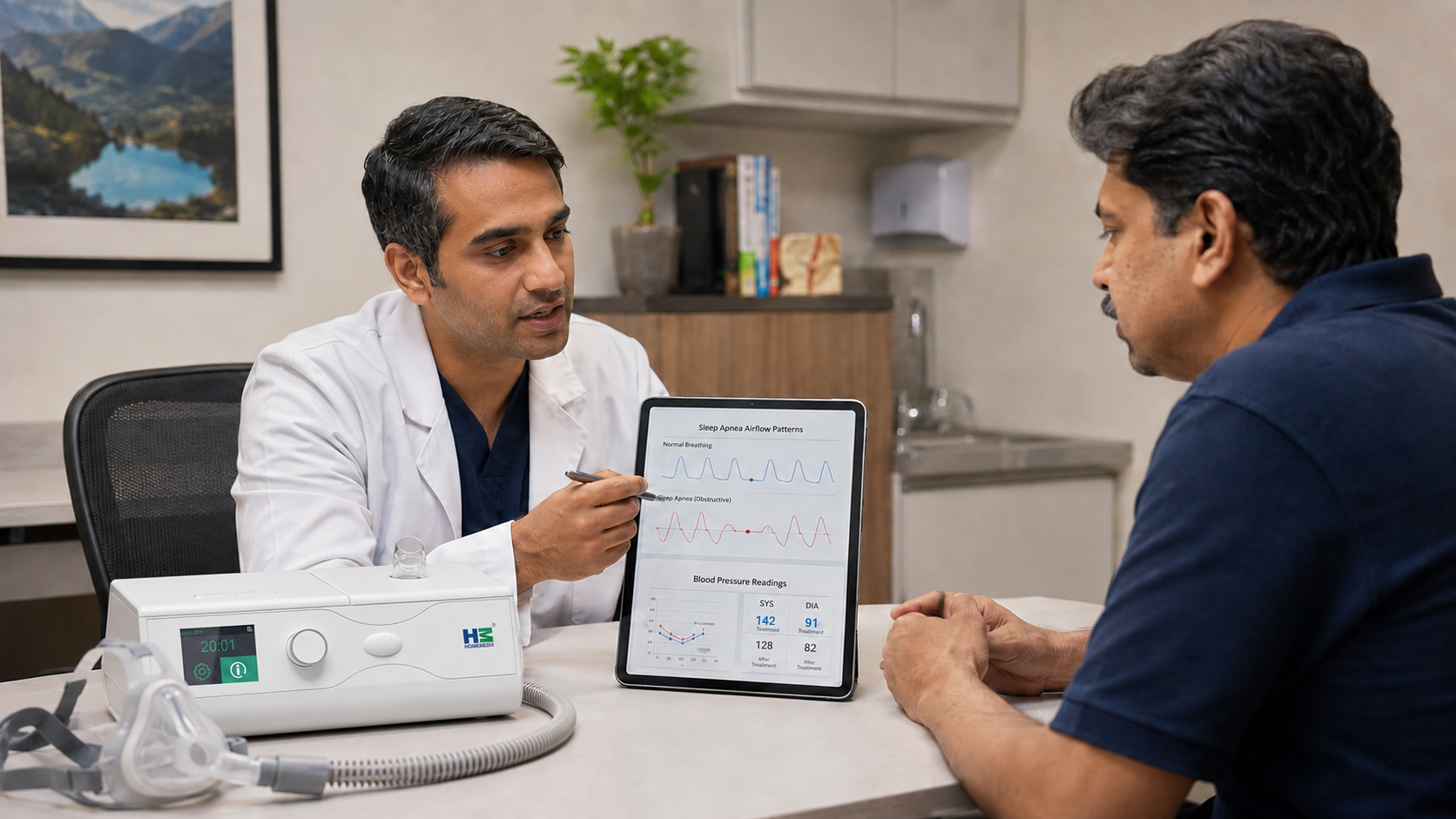
Does CPAP lower blood pressure: what the meta-analyses actually show
“Does CPAP lower blood pressure” is one of the most common questions an OSA patient asks after a fresh diagnosis, and the honest answer requires distinguishing average effect from individual response, and distinguishing CPAP used adequately from CPAP used nominally. The published meta-analyses converge on a modest average blood-pressure reduction of roughly 2–3 mmHg systolic. The tails